A.L.P. Fusion - Anterior/Lateral/Posterior Fusion
(ALIF/LLIF/PSF)
Surgical treatment to relieve back and leg pain caused by disc degeneration, spinal stenosis, instability and spinal deformity (scoliosis).
Interbody fusion is a surgical procedure that removes a painful lumbar disc and replaces it with a device to allow bone to grow across the disc space creating a fusion. The device stabilizes the collapsed and degenerated disc and restores stability to the segment, decreasing spinal pain. ALIF is done through a small incision in the lower abdomen and the spine is approached from the front. LLIF is done through a small incision in the side of the abdomen. Posterior fusion is done from the back.
If you have decided to have surgery:
- Call Dr. Jeffords' staff to schedule your surgery date and the pre-operative consultation.
- At your pre-operative consultation Dr. Jeffords or his staff will discuss the procedure with you, answer any questions you may have, and have you sign a consent form for surgery.
- You will be given prescriptions for pain medicine and instructions for post-operative care.
- Your pre-operative evaluation at the hospital or surgery center will be scheduled on the same day as your pre-operative consultation. You may have a chest X-ray, EKG, and blood-work performed.
- If you take aspirin or anti-inflammatory medications daily, STOP these medications at least 7 days before your surgery.
- If you are a smoker you should make every effort to stop smoking as soon as you can before surgery (at least 2 weeks prior to surgery). You should not smoke for at least 6 weeks after surgery.
- You will check into the hospital or surgery center the morning of surgery.
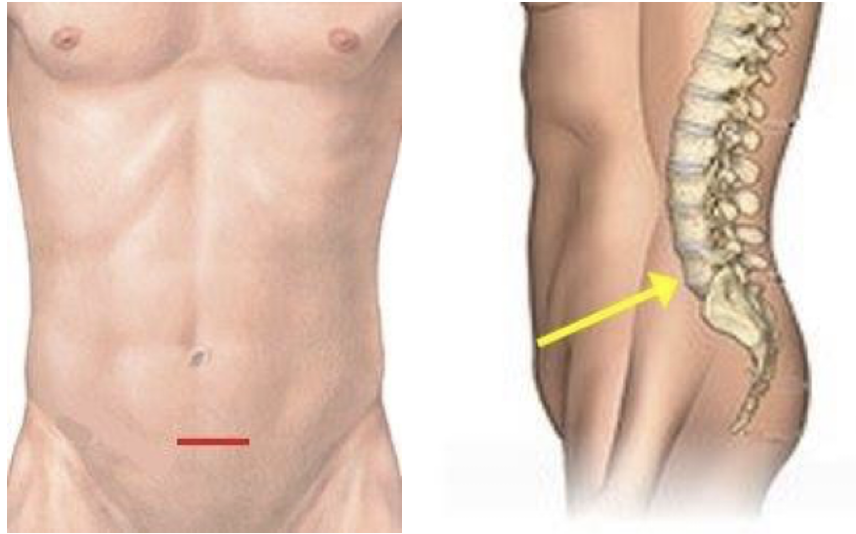
Anterior (Front) Procedure: ALIF
- Your anesthesiologist will bring you to the operating room and put you to sleep for the operation.
- You will be positioned lying on your back.
- ALIF is done through an either horizontal or vertical incision that is made on the front of your lower abdomen.
- The abdominal muscles are not cut, simply moved to the side.
- The abdominal contents are gently moved and a pathway from the skin to the spine is created, and retractors are placed to maintain the exposure of the spine.
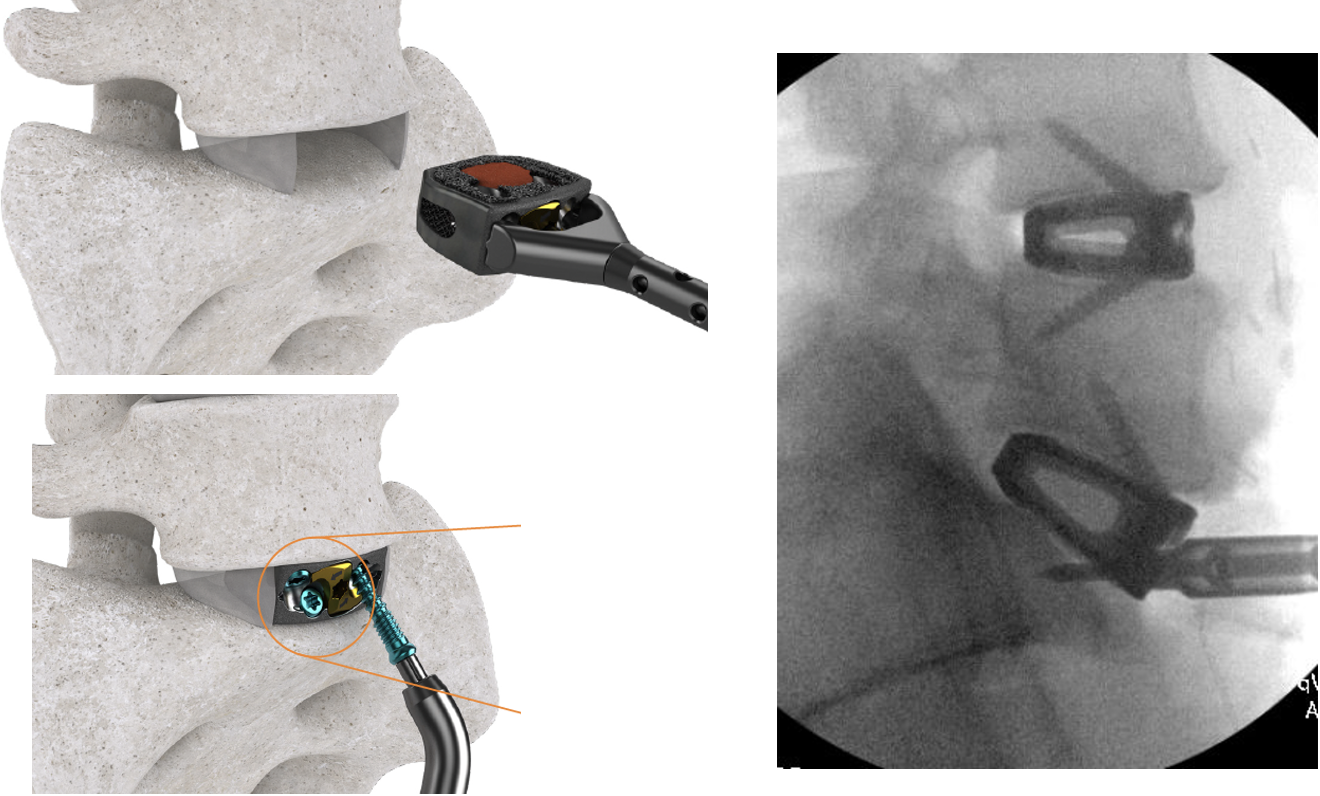
- Special instruments are used to remove the painful, degenerated disc and bone spurs (excess bone growth due to arthritis) to take pressure off of the nerves.
- The degenerated disc is then replaced with a fusion cage made of titanium and filled with bone graft.
- Screws may be placed through the device into the bones above and below, or a separate plate may be placed with screws that go through the plate into the bones.
- The retractor is removed, and the incision is closed with resorbable stitches that are placed beneath the skin.
- Typically, the ALIF is done at L5-S1 and sometimes L4-5.
Lateral (Side) Procedure: XLIF (also called LLIF)
- You will be positioned lying on your side.
- XLIF is done through a one inch incision that is made on the side of your abdomen between the ribcage and the pelvis.
- A series of tubes (dilators) are placed through the incision, one over the other through the muscle tissue onto the bones of the spine.
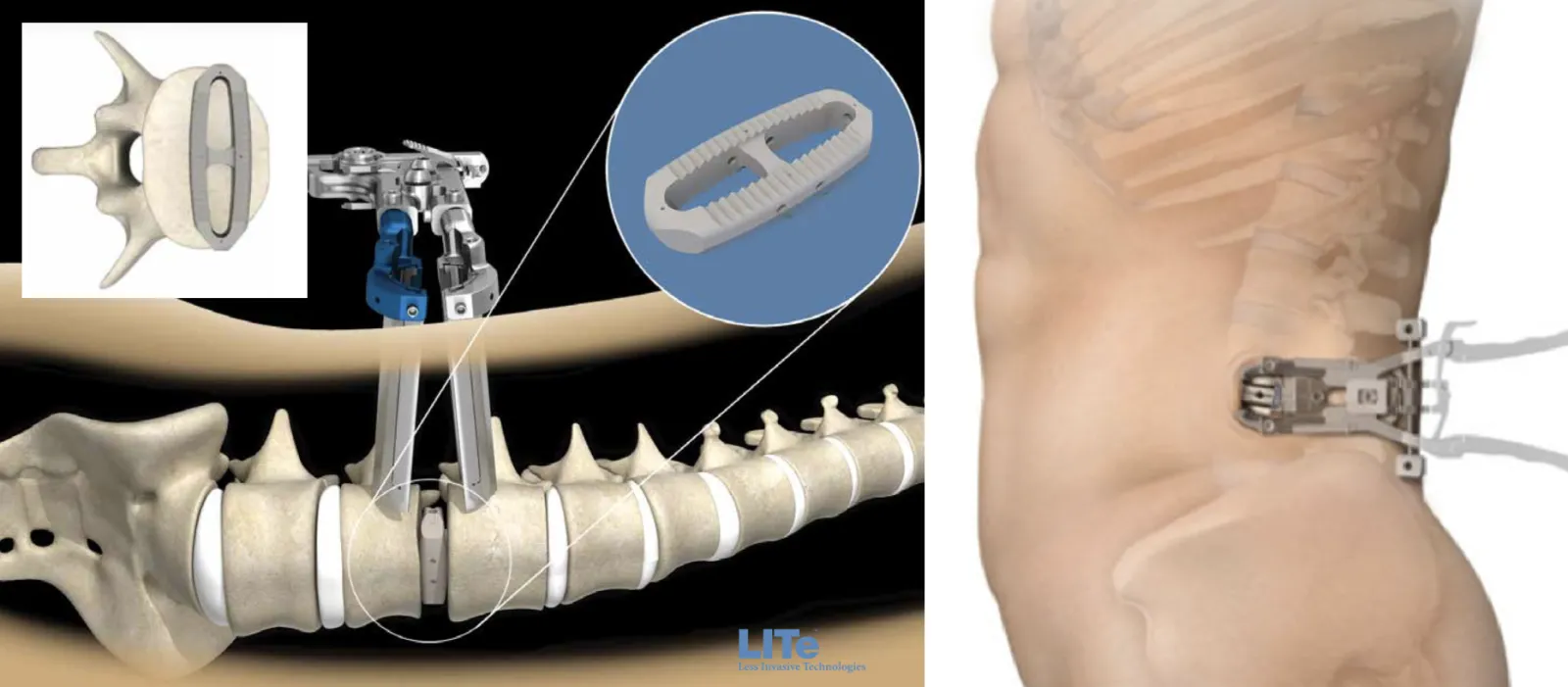
- A tubular retractor is placed over the dilators which are then removed. The tubular retractor is typically the diameter of a half-dollar and serves as a working channel or portal that the surgeon can perform the surgery through, leaving the muscle tissue intact. This minimizes incisional pain and scarring of the muscles.
- Special instruments are used to work through the tube to remove the painful, degenerated disc and bone spurs (excess bone growth due to arthritis) to take pressure off of the nerves.
- The degenerated disc is then replaced with a fusion cage made of either a special plastic called PEEK or titanium and filled with bone graft.
- The retractor is removed, and the incision is closed with resorbable stitches that are placed beneath the skin.
- Typically, for the A.L.P. fusion, the LLIF will be performed at L2-3, L3-4 and L4-5.
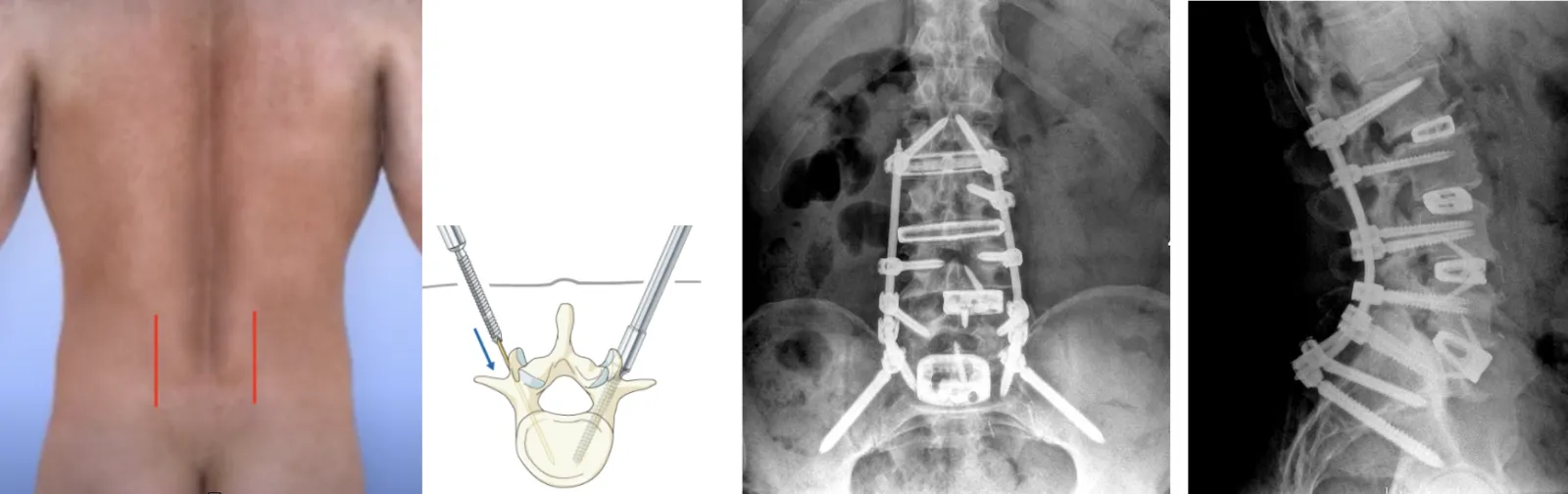
Posterior (Back) Procedure: Pedicle Screw Insertion:
- The ALIF and XLIF cages will be given extra support by placing screws and rods into the bones of the spine from the back (posterior).
- Sometimes this part of the surgery is done on a separate day than the ALIF and XLIF.
- For this part of the procedure, you will be repositioned on the table lying face down.
- Multiple small incisions will be made and X-ray or CT imaging is used to guide the screws through the small incisions into the bones that are above and below each of the fusion cages that were placed.
- If the fusion needs to extend into the thoracic spine, sometimes a six-inch incision is made to put bone graft onto the bones in that area and to place additional screws.
- The screws are then connected by rods to hold the spinal bones in their correct alignment as they heal and fuse through the ALIF and XLIF cages.
- The screws and rods will be placed from the top bone being fused down to the bottom bone being fused, typically S1. Sometimes screws are also placed into the pelvis through S2 to provide additional stability and fixation to prevent screw loosening.
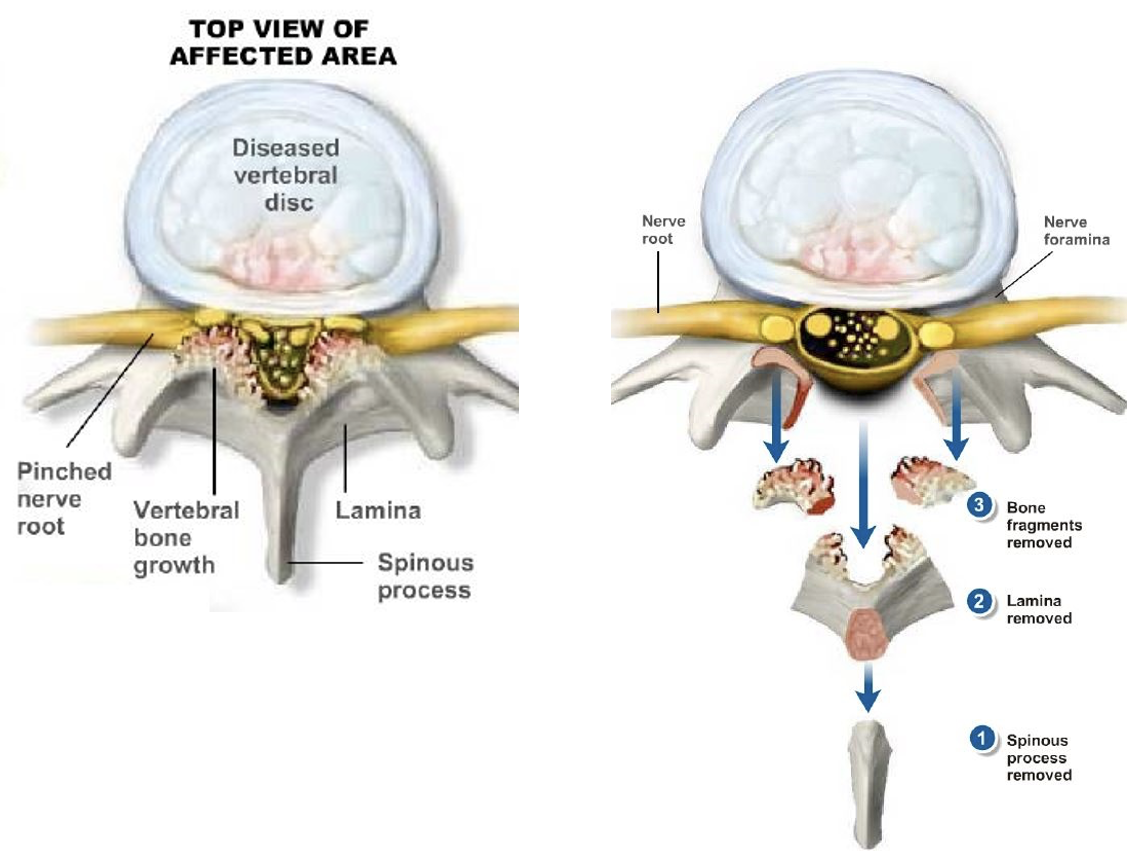
Laminectomy (if needed)
- In some cases, additional work will be needed to remove all of the bone spurs that are causing the narrowing (stenosis) of the spinal canal.
- A 1-2 inch incision is made in middle of your lower back. After carefully moving the muscle tissue, a small retractor is placed to expose the back of the spine.
- The bone and ligament tissue forming the "rooftop" of the spinal canal is removed to relieve pressure on the nerves.
Final Result:
- Removing the degenerated disc material and placing the ALIF and XLIF cages and screws and rods can achieve the following goals:
- Improves the height and proper alignment of the collapsed disc spaces, correcting spinal deformity (scoliosis) and spinal instability (spondylolisthesis)
- Allows for removal of pressure on the nerves, relieving radiating leg pain
- Provides biomechanical stability to the bones as they are fusing, reducing the incidence of screw loosening
- Increases the chances that the fusion will heal successfully
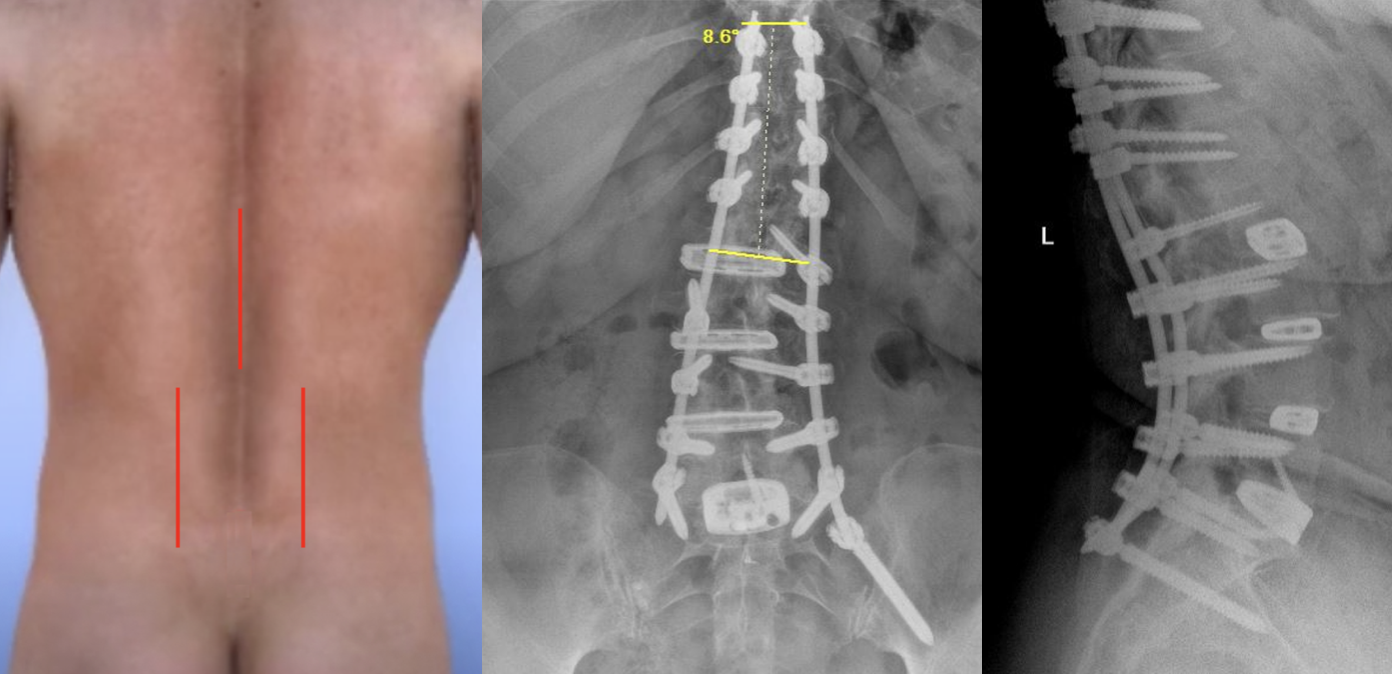
Before:
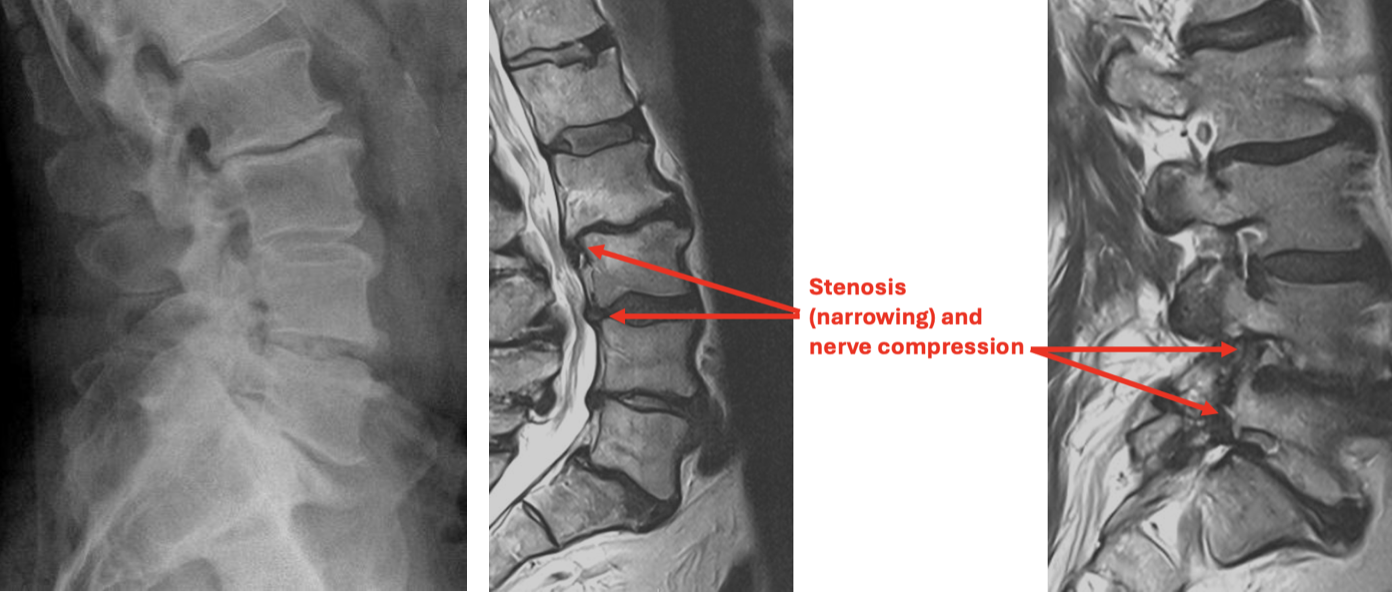
After:
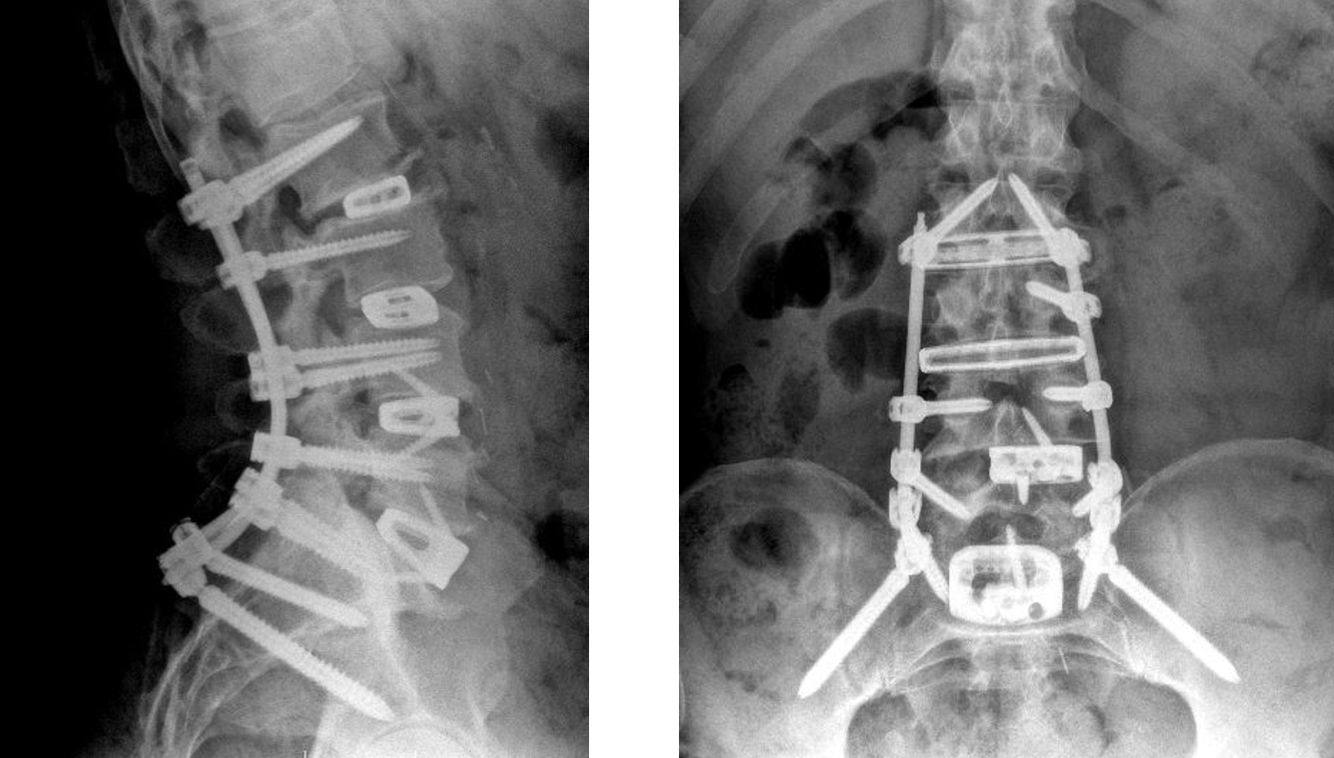
Scoliosis Correction:
- In some cases as the lumbar discs degenerate they collapse more on one side creating angular deformity and scoliosis (curvature of the spine).
- Placing the cages creates a parallel space between the bones, correcting the scoliosis.
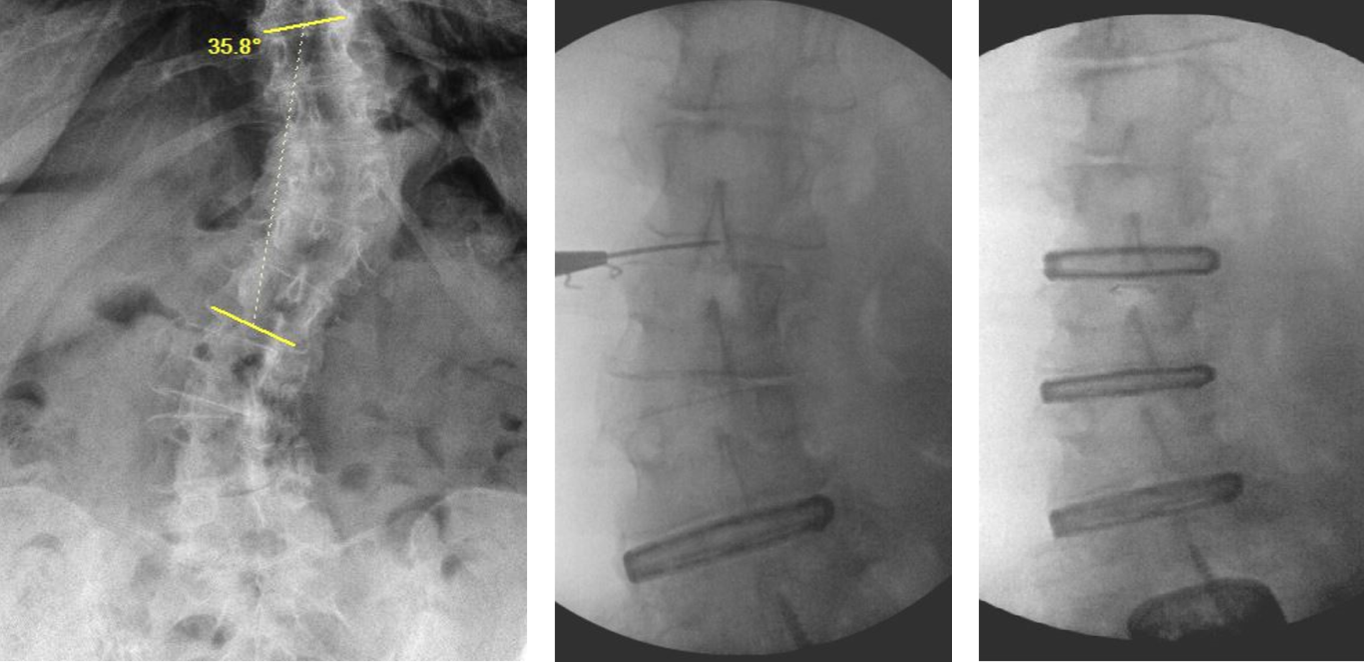
- Further correction of the scoliosis is achieved with the screws and rods.
- In some cases the fusion will be taken up to the T10 level with the screws and rods.
After Surgery:
- You will be taken to the recovery room (PACU) and stay there for about 1-1 ½ hours.
- Dr. Jeffords will speak to your family while you are in the recovery room.
- The nurses will get you out of bed shortly after surgery and a physical therapist may work with you to ensure that you are able to walk and climb stairs.
- Many patients go home the day of surgery. Some patients stay overnight and go home the morning after surgery.
- You will be able to ride in a car or plane upon leaving the surgery center or hospital.
After Going Home:
- A small waterproof dressing is placed over the incision in the operating room. You may shower over the dressing beginning the day after surgery. The dressing should be removed 7 days after surgery. After that, you may shower over the steri-strips covering the incision.
- For the first three months, avoid excessive bending or twisting at the waist. Some minor bending and twisting is acceptable.
- You should not lift more than 20 lbs for the first three months.
- You will be given pain medication and a muscle relaxant to help control post-operative pain and spasms. Make sure you do not drive or operate heavy machinery while on the medication.
- You may drive after 2-3 weeks, once you are off of your pain medications.
- You can expect to return to sedentary office or desk work approximately 2-3 weeks after surgery.
- You will have a post-operative office visit with Dr. Jeffords' team 2 weeks after surgery and again at 3 months and 6 months.
- You will begin a physical therapy program for back strengthening and flexibility 3-6 months after surgery when the fusion is healed.
- If you perform manual labor that requires heavy lifting or frequent bending or climbing you should wait 3-6 months before returning to this activity.
- Sports activities such as golf or tennis may be resumed at 3-6 months if the fusion is solid.